
Thursday, December 24, 2009
Mechanical Forage
The profitability of rotational grazing versus mechanical harvesting of forages was estimated using data from 237 nongrazing and 57 grazing farms participating in the New York farm business summary program in the year 2000. The objective was to perform an empirical comparison of the profitability of grazing versus mechanical forage harvesting systems. A regression analysis technique that controls for treatment selection bias is used to determine the impact of grazing on the rate of return on assets. This is accomplished by joint maximum likelihood estimation of a probit adoption function and a profit function. The results indicate that treatment selection does not have an important impact on the estimate of the profitability of grazing. There were wide ranges and overlap of profitability among herds using the two systems. However, other things equal, farmers utilizing grazing systems were at least if not more profitable than farmers not using grazing systems. After controlling for the factors influencing the decision to graze, we found that herd size, rate of milk production per cow, and prices received for milk have a strong positive impact on profitability. Farmers who perceive potential lifestyle benefits that might be obtained by implementing a grazing system likely do not have to pay an income penalty for adopting a grazing system.
The mechanical basis for airway hyperreactivity
New perspectives on the mechanical basis for airway hyperreactivity and airway hypersensitivity in asthma
We revisit the airway wall model of Lambert et. al. (Lambert RK, Wiggs BR, Kuwano K, Hogg JC, and Pare PD. J Appl Physiol 74: 2771–2781, 1993). We examine in detail the notion of a general airway bistability such that the airway lumen can suddenly decrease from a relatively open to a relatively closed condition without needing additional increase in active airway smooth muscle (ASM) tension during the stimulation. The onset of this bistability is an emergent consequence of the balance of forces associated with airway wall properties, parenchymal tissue properties, maximum lung elastic recoil, and the maximum stress that the ASM can generate. In healthy lungs, we find that all these properties reside in conditions that largely prevent the emergence of the bistability even during maximum ASM stimulation. In asthmatic airways, however, the airway wall and ASM remodeling conditions can tip the balance so as to promote the onset of the bistability at a lower dose of ASM stimulation (enhanced sensitivity) and then work to amplify the maximum constriction reached by each airway (enhanced reactivity). Hence, a larger fraction of asthmatic airways can display overall airway hyperreactivity. Simulations studies examine the role of increasing ASM maximum tension, airway wall stiffening, reduced lung volume, and decreased parenchymal tethering. Results predict that the single most important factor causing this airway hyperreactivity is amplified maximum ASM tension and not a thickening of the airway wall per se.
airway walls; airway remodeling
Monday, December 14, 2009
MECHANICAL FACTORS
1. The lymph of the thoracic duct furnishes to the blood a larger proportion than is usually supposed of the lymphocytes in circulation. Gross variations in its output of such cells must affect very considerably the blood picture.
2. The quantity of lymphocytes supplied through the thoracic duct of the healthy dog remains practically constant from hour to hour, if the physiological conditions are not notably changed. Transient change in physiological conditions may alter the output of cells, but with the disappearance of this change the output tends to resume its previous rate. These facts indicate that the tissues producing lymphocytes are "set" at a rate of activity definite in the individual.
3. Muscular activity (struggle) produces a prompt increase in the output of lymphocytes through the thoracic duct.
(a) This is assured by the presence of an increased number of cells per cubic millimeter of lymph, combined with an increase in the amount of lymph voided.
(b) The lymphocyte-output may be tripled or quadrupled during a long-continued struggle.
(c) Following prolonged struggle the output of lymphocytes is for a short time less than previous to the exertion.
4. The increased lymph-flow caused by a lymphagogue of the second class (glucose) brings with it increased output of lymphocytes through the thoracic duct.
(a) The individual cubic millimeters of lymph are often poor in cells, during the rapid lymph-flow, yet the total number of elements transported is large.
(b) The results with glucose support the theory of Ehrlich, that a rapidly appearing lymphocytosis may be produced through the flushing effect of increased lymph-flow.
5. A comparison of the effects of struggle with those of glucose demonstrates that in the former some factor besides increase in lymph-flow per se (Ehrlich) works to cause the large output of lymphocytes. The nature of this factor has not yet been determined.

6. The variations caused by muscular exertion and by increased lymph-flow in the number of lymphocytes coursing through the thoracic duct are so pronounced as to suggest that the total number of lymphocytes in circulation must be considerably influenced by them. Clinical findings by other observers indicate that this is true; and the clinical findings themselves become much simpler of interpretation.
7. The results in general prove the existence, reserved from circulation, of a large fund of lymphocytes, which is quickly yielded to the blood under certain physiological conditions
Friday, December 11, 2009
Probe into poison boiler
Tenants Derek Cookson, 77, along with wife Joyce, 79, of Danes Close, were exposed to deadly fumes after repeated calls to Gedling Homes about the boiler being broken.
Mrs Cookson was rushed to hospital and Mr Cookson was left on the verge of collapse.
Now Gedling Homes has brought in an independent surveyor who is investigating the cause of the leak, alongside the Health & Safety Executive.
The charity National CO-Gas Safety had yesterday called for an independent investigation.
Stephanie Trotter president and director of CO-Gas Safety, said they have been monitoring the couple's situation since they read their story in the Evening Post.
The charity has campaigned for increased awareness about the threat of carbon monoxide poisoning since 1995.
Only CORGI engineers are allowed to work on gas appliances by law. No similar rules exist for those who have solid fuel burners, like the one in the Cooksons' home.
Mrs Trotter said: "We have always lobbied that solid fuel engineers should be registered by law."
On November 29, records left by an engineer who visited the Cooksons stated he was not trained to deal with solid fuel burners. Their daughter, Carole had already explained what type of boiler her parents had.
Jim Lambeth, general manager of advisory service, The Solid Fuel Association, said: "From the pictures I have seen the boiler is clearly in a poor state and vital maintenance has not been carried out.
"In any rented property, it's the responsibility of the landlord to maintain the boiler to keep it in working order and it's the tenant's responsibility to carry out routine maintenance.
"HETAS are a group who hold a list of approved solid fuel engineers but effectively anyone can be employed to service a solid fuel boiler. That's the problem, a council can employ anyone legally to do the job."
Lynne Clayton, managing director at Gedling Homes, said: "We are working hard to get Mr and Mrs Cookson back to their home. Specialist contractors are working today to ensure they can return safely which will be before the weekend. Temporary heating and hot water are in place. With Mr Cookson's agreement, a gas meter is being installed, and we will put in a new central heating system."
Mr Cookson, an ex-miner, used anthracite to fuel his boiler. A hard, compact variety of mineral coal, it can leave a residue in the flue of a boiler and if this is not properly maintained, it can lead to a blockage and fume leaks containing carbon monoxide
Thursday, December 10, 2009
Control of cell membrane tension by myosin-I
Abstract
All cell functions that involve membrane deformation or a change in cell shape (e.g., endocytosis, exocytosis, cell motility, and cytokinesis) are regulated by membrane tension. While molecular contacts between the plasma membrane and the underlying actin cytoskeleton are known to make significant contributions to membrane tension, little is known about the molecules that mediate these interactions. We used an optical trap to directly probe the molecular determinants of membrane tension in isolated organelles and in living cells. Here, we show that class I myosins, a family of membrane-binding, actin-based motor proteins, mediate membrane/cytoskeleton adhesion and thus, make major contributions to membrane tension. These studies show that class I myosins directly control the mechanical properties of the cell membrane; they also position these motor proteins as master regulators of cellular events involving membrane deformation.
Wednesday, December 9, 2009
Post-Tensioning Revisited
Post-tensioned concrete has been used for more than 40 years in the United States in a wide variety of construction projects. First used primarily in bridge construction, applications for post-tensioning now extend far beyond bridges to include tanks, office buildings, condominiums, hotels, parking structures, pavement, masonry, seismic walls, single-family homes and more. Because post-tensioning can be combined effectively with other structural materials and has been used to strengthen steel, reinforced concrete, masonry and timber structures, as well as enhance and extend the capabilities of precast, pre-tensioned elements- the method's usage will continue to increase.
One reason for the increasing use of post-tensioning is the advancement in technology in recent years. While older post-tensioning systems focused more on obtaining the desired prestress force and less on durability, by improving the systems used to protect the prestressed steel from corrosion, the industry can now offer systems that deliver both. The advancements in corrosion protection are especially important in areas that experience significant exposure and damage from freeze-thaw cycles, de-icing salts, seawater, salt spray and other deterioration mechanisms.
Post-Tensioning Vs. Pre-Tensioning
Both pre-tensioning and post-tensioning systems are used to create prestressed concrete. Pre-tensioned systems, however, must be fabricated in a precast plant and are limited to straight, harped or circular tendons. This method is also limited to straight or circular members. Because pre-tensioning is used only in precast elements, it is more difficult to construct continuous structures because of the necessary connections. Additionally, though the tendons in pre-tensioned concrete are protected from corrosion because they are in direct contact with concrete, the steel itself is not able to be encapsulated in any other manner. As such, any moisture migrating to the steel through cracks in the concrete could cause the tendons to corrode.
Post-tensioning, on the other hand, can be performed on the project site or in a precast yard. Post-tensioning tendons can be configured into almost any shape. This flexibility allows the post-tensioning to match exact design requirements with few limitations. And, depending on project needs, the tendons in a post-tensioned system can be unbonded or bonded. For corrosion protection, whether unbonded or bonded - post-tensioning has superior features
Unbonded and Bonded Post-Tensioning Systems
Unbonded tendons typically consist of single (mono) strands or threaded bars that remain unbonded to the surrounding concrete throughout their service life - giving them freedom to move locally relative to the structural member. The strands in unbonded monostrand systems are coated with specially formulated grease with an outer layer of seamless plastic extruded in one continuous operation to provide protection against corrosion. Depending on the application and the level of protection that is needed, the anchorages of unbonded monostrand systems may also be encapsulated. Unbonded monostrand systems are typically used in new construction for elevated slabs, slabs-on-grade, beams and transfer girders, joists, shear walls and mat foundations. Light and flexible, unbonded monostrand can be easily and rapidly installed - providing an economical solution.
Bonded post-tensioning systems are comprised of tendons from one to multiple strands (multistrand) or bars. For bonded systems the prestressing steel is encased in a corrugated metal or plastic duct. After the tendon is stressed, cementitious grout is injected into the duct to bond it to the surrounding concrete. In addition, the grout creates an alkaline environment which provides corrosion protection for the prestressing steel. An advanced duct system, PT-PlusTM, encases the prestressing steel in a corrugated duct and plastic coupler system.
Bonded strand post-tensioning systems can range from a single strand to 55 or more strands in a single tendon, while the anchorage assembly consists of local zone confinement reinforcement, bearing plate, anchor head, wedges and grout cap. Bonded multistrand systems, while used extensively in new construction of bridges and transportation structures, can be and have been successfully applied to commercial building structures. When these multistrand systems are used for large structural elements such as beams and transfer girders, design advantages include increased span lengths and load-carrying capacity and reduced deflection.
External and Internal Post-Tensioning
Tendons placed in the formwork prior to pouring the concrete are known as internal tendons. Most post-tensioning applications use internal tendons. In external applications, tendons are installed outside of the structural member. The system consists of prestressing steel, mechanical end anchorage devices and a corrosion protection system. External systems are generally installed in one of two configurations - either running straight between anchorages or through deviators to create harped profiles. The tendons are typically protected by high density polyethylene (HDPE) ducts filled with grout.
External systems, if designed accordingly, make it possible to control and adjust tendon forces, inspect for corrosion and, as necessary, easily replace the tendons. For these reasons, the primary application for external tendons is bridges where external multistrand systems are grouted in HDPE ducts. External tendon systems, however, can be applied to many types of structures and, in particular, provide effective strengthening reinforcement for retrofits.
Past Challenges Inspire Technological Advancement
Since post-tensioning was first used domestically, the industry has seen many technological advances. Improvements in systems include seven-wire strand with wedge-type anchorages, low relaxation strand and the use of banded tendons in flat plates. Analysis techniques and design software have advanced as have techniques for improving durability. These include extruded sheathing for unbonded tendons and encapsulated anchorages for enhanced corrosion resistance, plastic duct systems and the development of non-bleed grouts.
When some of the earliest unbonded post-tensioned buildings were about 15 years old, corrosion problems started to surface, and it was apparent that some of the tendon corrosion protection systems used could not adequately protect the tendons in the most aggressive environments, such as where de-icing salts are used or in coastal areas that have a high salt content in the air. Starting in the 1980s, the Post-Tensioning Institute (PTI) developed tendon specifications designed to address the corrosion problems. PTI specified improvements included sheathing, coatings and, in the most aggressive environments, complete encapsulation of the tendons.
With internal bonded and external tendons, grout is a key element of the overall corrosion protection strategy. Experience gained over many decades with grouted post-tensioning tendons has proven that cementitious grout provides excellent protection for the prestressing steel. The principle objectives of grouting are to protect the prestressing steel from corrosion by encasing it in a passive environment and filling the duct to minimize voids in the completed structure. To ensure the quality of grouting applications, and the ultimate durability of the structure, in addition to other training classes and certification programs, PTI developed and administers grout training classes and certification procedures. Specialized equipment has also been developed to complement the process and ensure the highest quality product.
Benefits of Post-Tensioned Concrete
Post-tensioned structures offer numerous advantages. These include reduced dead load and member depth because of the decreased amount concrete required. There is also increased deflection control and greater crack control. The improved crack control also improves durability which is another advantage. In addition to these advantages, post-tensioning allows for increased span to depth ratios. This advantage leads to lower building heights which in turn reduces the heating and cooling volume and decreases the façade area of the structure.
For developers and owners of commercial buildings, the advantages of post-tensioning can make it a preferred reinforcing system. "Since the slab thickness is reduced, a developer building a high rise structure can easily add more floors without increasing the overall building height," said Scott Greenhaus, president of VSL. "Over the course of the building's life, this can represent significantly increase leasing revenue for the owner."
A traditional reinforced concrete building with two-way slabs requires more concrete and thus, more weight. As a lighter alternative, post-tensioned slabs require less concrete to achieve the same performance, thereby creating a structure with fewer shear walls, smaller columns and lower foundation loads. This results in more durable, efficient structures with longer clear spans.
"For commercial building operators, residential developers and hotel operators, they can have more usable space within the building envelope," Greenhaus noted.
Further, in corrosive environments, encapsulated bonded systems offer significant design advantages that lead to life-cycle savings. Because the amount of mild steel is reduced, particularly at the top zone of slabs, there is less steel to corrode should the concrete crack or spall. This is particularly important in parking garages where significant maintenance costs are due to repairs associated with spalled concrete from corroded rebar.
Another advantage of bonded post-tensioning is the inherent capacity to provide resistance to progressive collapse. This may be especially important in the event of localized blast loading. Like mild steel reinforcement, a bonded post-tensioning tendon is capable of developing its force in a relatively short distance along its length. In the event that an anchorage fails or a tendon is severed, the loss of tendon force would be localized. The remainder of the tendon would retain its force at the development length away from the failure point and would remain functional. This functionality can be considered in the design of a structure.
Bonded post-tensioning systems also allow for flexibility when future modifications to the building are needed. Tenant build-outs, remodeling and changes in a building's use may require modifications to the floor slabs. The use of bonded post-tensioning systems has allowed owners the flexibility to make these changes quickly, easily and cost-efficiently.
An example of an owner choosing bonded post-tensioning for the method's life-cycle savings is the Baltimore Washington International Airport Consolidated Rental Facility. The bonded post-tensioning system used in this structure provides total encapsulation of the strands using PT PlusTM plastic duct with watertight mechanical duct to anchorage couplers. The rental facility was completed in December 2003 and includes over one million square feet of elevated, post-tensioned, cast-in-place concrete.
Bonded and unbonded systems can be mixed within a structure. An example of how bonded and unbonded systems were combined for economics, efficiency and design requirements is the W Victory Hotel & Residences in Dallas, Texas. The W Victory's concrete frame structure includes a combination of monostrand, unbonded post-tensioning systems and bonded, multistrand post-tensioning systems. The unbonded post-tensioned systems were used in typical levels, while the bonded post-tensioning systems were specified for the transfer girders on three levels to provide optimum crack and deflection control -- features essential for transfer girders required to carry the loads from the multi-story structure. Additionally, bonded post-tensioning systems were used in exterior applications where corrosion could be an issue.
Post-tensioning has seen much development and many improvements over the past 50 years, resulting in the method now serving as a significant feature in mainstream construction. The next article in this series will review in-depth the contemporary uses of post-tensioning in building construction and how it can successfully be incorporated into a project design.
Reasons to Consider Post-Tensioning
One reason for the increasing use of post-tensioning is the advancement in technology in recent years. While older post-tensioning systems focused more on obtaining the desired prestress force and less on durability, by improving the systems used to protect the prestressed steel from corrosion, the industry can now offer systems that deliver both. The advancements in corrosion protection are especially important in areas that experience significant exposure and damage from freeze-thaw cycles, de-icing salts, seawater, salt spray and other deterioration mechanisms.
Post-Tensioning Vs. Pre-Tensioning
Both pre-tensioning and post-tensioning systems are used to create prestressed concrete. Pre-tensioned systems, however, must be fabricated in a precast plant and are limited to straight, harped or circular tendons. This method is also limited to straight or circular members. Because pre-tensioning is used only in precast elements, it is more difficult to construct continuous structures because of the necessary connections. Additionally, though the tendons in pre-tensioned concrete are protected from corrosion because they are in direct contact with concrete, the steel itself is not able to be encapsulated in any other manner. As such, any moisture migrating to the steel through cracks in the concrete could cause the tendons to corrode.
Post-tensioning, on the other hand, can be performed on the project site or in a precast yard. Post-tensioning tendons can be configured into almost any shape. This flexibility allows the post-tensioning to match exact design requirements with few limitations. And, depending on project needs, the tendons in a post-tensioned system can be unbonded or bonded. For corrosion protection, whether unbonded or bonded - post-tensioning has superior features
Unbonded and Bonded Post-Tensioning Systems
Unbonded tendons typically consist of single (mono) strands or threaded bars that remain unbonded to the surrounding concrete throughout their service life - giving them freedom to move locally relative to the structural member. The strands in unbonded monostrand systems are coated with specially formulated grease with an outer layer of seamless plastic extruded in one continuous operation to provide protection against corrosion. Depending on the application and the level of protection that is needed, the anchorages of unbonded monostrand systems may also be encapsulated. Unbonded monostrand systems are typically used in new construction for elevated slabs, slabs-on-grade, beams and transfer girders, joists, shear walls and mat foundations. Light and flexible, unbonded monostrand can be easily and rapidly installed - providing an economical solution.
Bonded post-tensioning systems are comprised of tendons from one to multiple strands (multistrand) or bars. For bonded systems the prestressing steel is encased in a corrugated metal or plastic duct. After the tendon is stressed, cementitious grout is injected into the duct to bond it to the surrounding concrete. In addition, the grout creates an alkaline environment which provides corrosion protection for the prestressing steel. An advanced duct system, PT-PlusTM, encases the prestressing steel in a corrugated duct and plastic coupler system.
Bonded strand post-tensioning systems can range from a single strand to 55 or more strands in a single tendon, while the anchorage assembly consists of local zone confinement reinforcement, bearing plate, anchor head, wedges and grout cap. Bonded multistrand systems, while used extensively in new construction of bridges and transportation structures, can be and have been successfully applied to commercial building structures. When these multistrand systems are used for large structural elements such as beams and transfer girders, design advantages include increased span lengths and load-carrying capacity and reduced deflection.
External and Internal Post-Tensioning
Tendons placed in the formwork prior to pouring the concrete are known as internal tendons. Most post-tensioning applications use internal tendons. In external applications, tendons are installed outside of the structural member. The system consists of prestressing steel, mechanical end anchorage devices and a corrosion protection system. External systems are generally installed in one of two configurations - either running straight between anchorages or through deviators to create harped profiles. The tendons are typically protected by high density polyethylene (HDPE) ducts filled with grout.
External systems, if designed accordingly, make it possible to control and adjust tendon forces, inspect for corrosion and, as necessary, easily replace the tendons. For these reasons, the primary application for external tendons is bridges where external multistrand systems are grouted in HDPE ducts. External tendon systems, however, can be applied to many types of structures and, in particular, provide effective strengthening reinforcement for retrofits.
Past Challenges Inspire Technological Advancement
Since post-tensioning was first used domestically, the industry has seen many technological advances. Improvements in systems include seven-wire strand with wedge-type anchorages, low relaxation strand and the use of banded tendons in flat plates. Analysis techniques and design software have advanced as have techniques for improving durability. These include extruded sheathing for unbonded tendons and encapsulated anchorages for enhanced corrosion resistance, plastic duct systems and the development of non-bleed grouts.
When some of the earliest unbonded post-tensioned buildings were about 15 years old, corrosion problems started to surface, and it was apparent that some of the tendon corrosion protection systems used could not adequately protect the tendons in the most aggressive environments, such as where de-icing salts are used or in coastal areas that have a high salt content in the air. Starting in the 1980s, the Post-Tensioning Institute (PTI) developed tendon specifications designed to address the corrosion problems. PTI specified improvements included sheathing, coatings and, in the most aggressive environments, complete encapsulation of the tendons.
With internal bonded and external tendons, grout is a key element of the overall corrosion protection strategy. Experience gained over many decades with grouted post-tensioning tendons has proven that cementitious grout provides excellent protection for the prestressing steel. The principle objectives of grouting are to protect the prestressing steel from corrosion by encasing it in a passive environment and filling the duct to minimize voids in the completed structure. To ensure the quality of grouting applications, and the ultimate durability of the structure, in addition to other training classes and certification programs, PTI developed and administers grout training classes and certification procedures. Specialized equipment has also been developed to complement the process and ensure the highest quality product.
Benefits of Post-Tensioned Concrete
Post-tensioned structures offer numerous advantages. These include reduced dead load and member depth because of the decreased amount concrete required. There is also increased deflection control and greater crack control. The improved crack control also improves durability which is another advantage. In addition to these advantages, post-tensioning allows for increased span to depth ratios. This advantage leads to lower building heights which in turn reduces the heating and cooling volume and decreases the façade area of the structure.
For developers and owners of commercial buildings, the advantages of post-tensioning can make it a preferred reinforcing system. "Since the slab thickness is reduced, a developer building a high rise structure can easily add more floors without increasing the overall building height," said Scott Greenhaus, president of VSL. "Over the course of the building's life, this can represent significantly increase leasing revenue for the owner."
A traditional reinforced concrete building with two-way slabs requires more concrete and thus, more weight. As a lighter alternative, post-tensioned slabs require less concrete to achieve the same performance, thereby creating a structure with fewer shear walls, smaller columns and lower foundation loads. This results in more durable, efficient structures with longer clear spans.
"For commercial building operators, residential developers and hotel operators, they can have more usable space within the building envelope," Greenhaus noted.
Further, in corrosive environments, encapsulated bonded systems offer significant design advantages that lead to life-cycle savings. Because the amount of mild steel is reduced, particularly at the top zone of slabs, there is less steel to corrode should the concrete crack or spall. This is particularly important in parking garages where significant maintenance costs are due to repairs associated with spalled concrete from corroded rebar.
Another advantage of bonded post-tensioning is the inherent capacity to provide resistance to progressive collapse. This may be especially important in the event of localized blast loading. Like mild steel reinforcement, a bonded post-tensioning tendon is capable of developing its force in a relatively short distance along its length. In the event that an anchorage fails or a tendon is severed, the loss of tendon force would be localized. The remainder of the tendon would retain its force at the development length away from the failure point and would remain functional. This functionality can be considered in the design of a structure.
Bonded post-tensioning systems also allow for flexibility when future modifications to the building are needed. Tenant build-outs, remodeling and changes in a building's use may require modifications to the floor slabs. The use of bonded post-tensioning systems has allowed owners the flexibility to make these changes quickly, easily and cost-efficiently.
An example of an owner choosing bonded post-tensioning for the method's life-cycle savings is the Baltimore Washington International Airport Consolidated Rental Facility. The bonded post-tensioning system used in this structure provides total encapsulation of the strands using PT PlusTM plastic duct with watertight mechanical duct to anchorage couplers. The rental facility was completed in December 2003 and includes over one million square feet of elevated, post-tensioned, cast-in-place concrete.
Bonded and unbonded systems can be mixed within a structure. An example of how bonded and unbonded systems were combined for economics, efficiency and design requirements is the W Victory Hotel & Residences in Dallas, Texas. The W Victory's concrete frame structure includes a combination of monostrand, unbonded post-tensioning systems and bonded, multistrand post-tensioning systems. The unbonded post-tensioned systems were used in typical levels, while the bonded post-tensioning systems were specified for the transfer girders on three levels to provide optimum crack and deflection control -- features essential for transfer girders required to carry the loads from the multi-story structure. Additionally, bonded post-tensioning systems were used in exterior applications where corrosion could be an issue.
Post-tensioning has seen much development and many improvements over the past 50 years, resulting in the method now serving as a significant feature in mainstream construction. The next article in this series will review in-depth the contemporary uses of post-tensioning in building construction and how it can successfully be incorporated into a project design.
Reasons to Consider Post-Tensioning
- Increased span to depth ratio resulting in a reduction in construction materials and a subsequent reduction in overall cost.
- Positive deflection control.
- Designers are offered design flexibility with post-tensioning.
- Joints in structures are minimized or even eliminated.
- Post-tensioning can improve the long-term durability of concrete structures exposed to aggressive environments.
- Span lengths can be greatly increased.
Monday, December 7, 2009
Basic concepts in mechanical ventilation

Wednesday, December 2, 2009
Ventilation, Mechanical
Ventilation, Mechanical
Background
The Drinker and Shaw tank-type ventilator of 1929 was one of the first negative-pressure machines widely used for mechanical ventilation. Better known as the iron lung, this metal cylinder completely engulfed the patient up to the neck. A vacuum pump created negative pressure in the chamber, which resulted in expansion of the patient's chest. This change in chest geometry reduced the intrapulmonary pressure and allowed ambient air to flow into the patient's lungs. When the vacuum was terminated, the negative pressure applied to the chest dropped to zero, and the elastic recoil of the chest and lungs permitted passive exhalation
Ventilation of the patient was accomplished without the placement of a tracheostomy or an endotracheal tube. Nevertheless, this mode of ventilation was cumbersome and led to patient discomfort. In addition, it limited access to the patient by health care providers. Because the negative pressure created in the chamber was exerted on the abdomen as well as the chest, the cardiac output tended to decrease from pooling of venous blood in the lower torso.Today, negative-pressure ventilation is used in only a few situations. The cuirass, or shell unit, allows negative pressure to be applied only to the patient's chest by using a combination of a form-fitted shell and a soft bladder. It provides a suitable and attractive option for patients with neuromuscular disorders, especially those with residual muscular function, because it does not require a tracheostomy with its inherent problems.
Concepts that the military developed during World War II to deliver oxygen and gas volume to fighter pilots operating at high altitude were incorporated into the design of the modern positive-pressure ventilator. With the development of safe endotracheal tubes with high-volume, low-pressure cuffs, positive-pressure ventilation replaced the iron lung.
Intensive use of positive-pressure mechanical ventilation gained momentum during the polio epidemic in Scandinavia and the United States in the early 1950s. In Copenhagen, the patient with polio and respiratory paralysis who was supported by manually forcing 50% oxygen through a tracheostomy had a reduced mortality rate. However, this heroic intervention required the continuous activity of 1400 medical students recruited from the universities. The overwhelming manpower needed, coupled with a decrease in mortality rate from 80% to 25%, led to the adaptation of the positive-pressure machines used in the operating room for use in the ICU.
Positive-pressure ventilation means that airway pressure is applied at the patient's airway through an endotracheal or tracheostomy tube. The positive nature of the pressure causes the gas to flow into the lungs until the ventilator breath is terminated. As the airway pressure drops to zero, elastic recoil of the chest accomplishes passive exhalation by pushing the tidal volume out.
Classifications of Positive-Pressure Ventilators
Modern ventilators are classified by their method of cycling from the inspiratory phase to the expiratory phase. That is, they are named after that parameter that signals the termination of the positive-pressure inspiration cycle of the machine. The signal to terminate the inspiratory activity of the machine is either a preset volume (for a volume-cycled ventilator), a preset pressure limit (for a pressure-cycled ventilator), or a preset time factor (for a time-cycled ventilator).
Volume-cycled ventilation is the most common form of ventilator cycling used in adult medicine because it provides a consistent breath-to-breath tidal volume. Termination of the delivered breath is signaled when a set volume leaves the ventilator.
Indications for Mechanical Ventilation
Many factors affect the decision to begin mechanical ventilation. Because no mode of mechanical ventilation can cure a disease process, the patient should have a correctable underlying problem that can be resolved with the support of mechanical ventilation. This intervention should not be started without thoughtful consideration because intubation and positive-pressure ventilation are not without potentially harmful effects.
Mechanical ventilation is indicated when the patient's spontaneous ventilation is inadequate to sustain life. In addition, it is indicated as a measure to control ventilation in critically ill patients and as prophylaxis for impending collapse of other physiologic functions. Physiologic indications include respiratory or mechanical insufficiency and ineffective gas exchange.
Common indications for mechanical ventilation include the following:
- Bradypnea or apnea with respiratory arrest
- Acute lung injury and the acute respiratory distress syndrome
- Tachypnea (respiratory rate >30 breaths per minute)
- Vital capacity less than 15 mL/kg
- Minute ventilation greater than 10 L/min
- Arterial partial pressure of oxygen (PaO2) with a supplemental fraction of inspired oxygen (FIO2) of less than 55 mm Hg
- Alveolar-arterial gradient of oxygen tension (A-a DO2) with 100% oxygenation of greater than 450 mm Hg
- Clinical deterioration
- Respiratory muscle fatigue
- Obtundation or coma
- Hypotension
- Acute partial pressure of carbon dioxide (PaCO2) greater than 50 mm Hg with an arterial pH less than 7.25
- Neuromuscular disease
The trend of these values should influence clinical judgment. Increasing severity of illness should prompt the clinician to consider starting mechanical ventilation.
Initial Ventilator Settings
Mode of ventilation
After deciding to start positive-pressure ventilation with a volume-cycled ventilator, the clinician must now select the safest initial mode of machine operation.
In most circumstances, the initial mode of ventilation should be the assist-control mode, in which a tidal volume and rate are preset and guaranteed. The patient can affect the frequency and timing of the breaths. If the patient makes an inspiratory effort, the ventilator senses a decrease in the circuit pressure and delivers the preset tidal volume. In this way, the patient can dictate a comfortable respiratory pattern and may trigger additional machine-assisted breaths above the set rate. If the patient does not initiate inspiration, the ventilator automatically delivers the preset rate and tidal volume, ensuring minimum minute ventilation. In the assist-control mode, the work of breathing is reduced to the amount of inspiration needed to trigger the inspiratory cycle of the machine. This trigger is adjusted by setting the sensitivity of the machine to the degree of pressure decrease desired in the circuit
The pressure, volume, and flow to time waveforms for assist-control ventilation.
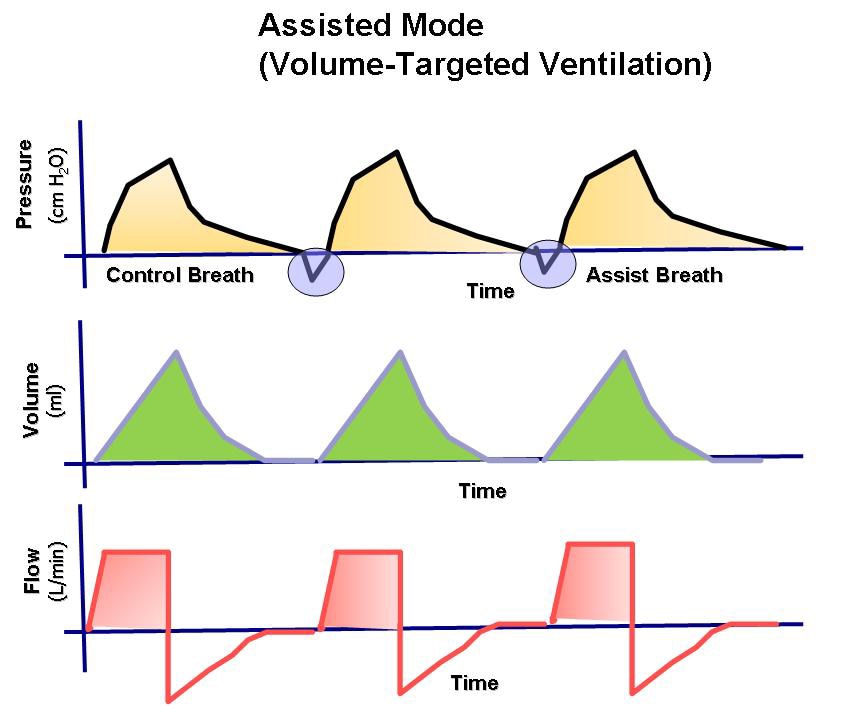
Assist-control differs from controlled ventilation because the patient can trigger the ventilator to deliver a breath and, thereby, adjust their minute ventilation. In controlled ventilation, the patient receives only breaths initiated by the ventilator at the preset rate
The pressure, volume, and flow to time waveforms for controlled ventilation.
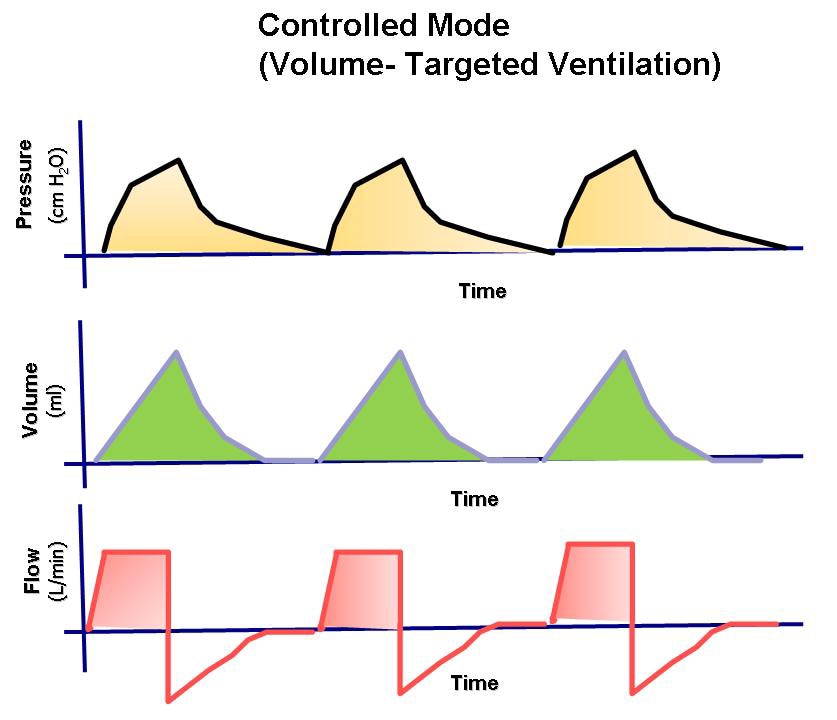
Although the work of breathing is not eliminated, this mode gives the respiratory muscles the greatest amount of rest because the patient needs only to create enough negative pressure to trigger the machine. An added advantage is that the patient can achieve the required minute ventilation by triggering additional breaths above the set back-up rate.
In most cases, a minute ventilation that provides a reasonable pH based on the respiratory rate is determined by the patient's chemoreceptors and stretch receptors. The respiratory center in the central nervous system receives input from the chemical receptors (arterial blood gas tensions) and neural pathways that sense the mechanical work of breathing (mechanoreceptors). The respiratory rate and respiratory pattern are the result of input from these chemoreceptors and mechanical receptors, which allow the respiratory center to regulate gas exchange. In the assist-control mode, this process is accomplished with the minimum work of breathing.
A second possible advantage of this mode of mechanical ventilation is that cycling the ventilator into the inspiratory phase maintains normal ventilatory activity and, therefore, prevents atrophy of the respiratory muscles.
A potential disadvantage of the assist-control mode is respiratory alkalosis in a small subset of patients whose respiratory drive supersedes the chemoreceptors and mechanical receptors. Patients with a potential for alveolar hyperventilation and hypocapnia in the assist-control mode include those with end-stage liver disease, those in the hyperventilatory stage of sepsis, and those with head trauma. These conditions are typically identified with the first arterial blood gas results, and the assist-control mode of ventilation can then be changed to an alternate mode.
Another possible disadvantage is the potential for serial preset positive-pressure breathes to retard venous return to the right side of heart and to affect global cardiac output. Nevertheless, the assist-control mode may be the safest initial choice for mechanical ventilation. It may be switched to another option if hypotension or hypocarbia are evident from the first arterial blood gas results.
Tidal volume and rate
For a patient without preexisting lung disease, the tidal volume and rate are traditionally selected by using the 12-12 rule. A tidal volume of 12 mL for each kilogram of lean body weight is programmed to be delivered 12 times a minute in the assist-control mode.
For patients with chronic obstructive pulmonary disease (COPD), the tidal volume and rate are slightly reduced to the 10-10 rule to prevent overinflation and hyperventilation. A tidal volume of 10 mL/kg lean body weight is delivered 10 times a minute in the assist-control mode.
In acute respiratory distress syndrome (ARDS), the lungs may function best and volutrauma is minimized with low tidal volumes of 6-8 mL/kg. Tidal volumes are preset at 6-8 mL/kg of lean body weight in the assist-control mode. This ventilatory strategy is called lung-protective ventilation. These lowered volumes may lead to slight hypercarbia. An elevated PCO2 is typically recognized and accepted without correction, leading to the term permissive hypercapnia. However, the degree of respiratory acidosis allowable is a pH not less than 7.25. The respiratory rate of the ventilator may need to be adjusted upward to increase the minute ventilation lost by using smaller tidal volumes.
Double-checking the selected tidal volume
After a tidal volume is selected, the peak airway pressure necessary to deliver a single breath should be determined. As the tidal volume increases, so does the pressure required to force that volume into the lung. Persistent breath-to-breath peak pressures greater than 45 cm water are a risk factor for barotrauma . The tidal volume suggested by the above rules may need to be decreased in some patients to keep the peak airway pressure less than 45 cm water
The components of mechanical ventilation inflation pressures. Paw is airway pressure, PIP is peak airway pressure, Pplat is plateau pressure.
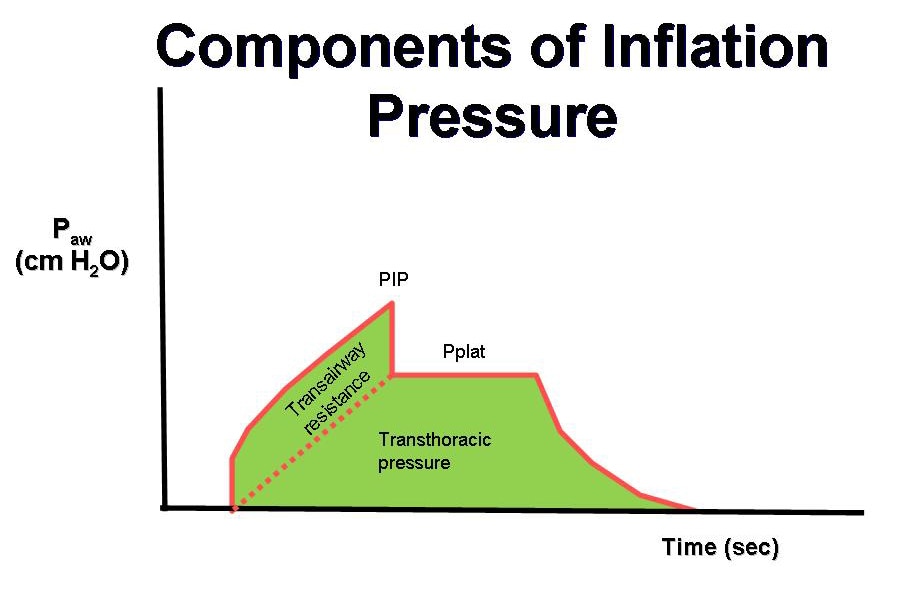
Some researchers have suggested that plateau pressures should be monitored as a means to prevent barotrauma in the patient with ARDS. Plateau pressures are measured at the end of the inspiratory phase of a ventilator-cycled tidal volume. The ventilator is programmed not to allow expiratory airflow at the end of the inspiration for a set time, typically half a second. The pressure measured to maintain this lack of expiratory airflow is the plateau pressure. Barotrauma is minimized when the plateau pressure is maintained at less than 30-35 cm water Monitoring the peak and plateau pressures allows physicians to make clinical judgments on the progress of their patient
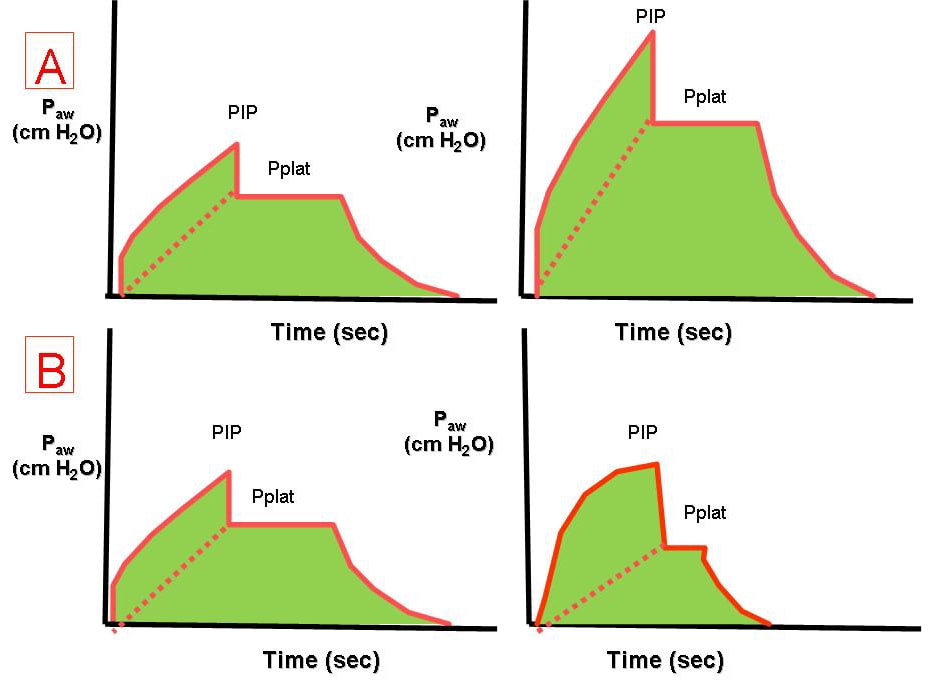
The effects of increased airway resistance (A) and decreased respiratory system compliance on the pressure-time waveform.
Sighs
Because a spontaneously breathing individual typically sighs 6-8 times each hour to prevent microatelectasis, some investigators once recommended that periodic machine breaths that were 1.5-2 times the preset tidal volume be given 6-8 times per hour. However, the peak pressure often needed to deliver such a volume was high enough to predispose the patient to barotrauma. At present, accounting for sighs is not recommended if the patient is receiving tidal volumes of 10-12 mL/kg or if the patient requires positive end-expiratory pressure (PEEP). When a low tidal volume is used, sighs are preset at 1.5-2 times the tidal volume and delivered 6-8 times an hour if the peak and plateau pressures are within acceptable limits.
Initial FIO2
The highest priority at the start of mechanical ventilation is providing effective oxygenation. For the patient's safety after intubation, the FIO2 should always be set at 100% until adequate arterial oxygenation is documented. A short period with an FIO2 of 100% is not dangerous to the patient receiving mechanical ventilation and offers the clinician several advantages. First, an FIO2 of 100% protects the patient against hypoxemia if unrecognized problems occur as a result of the intubation procedure. Second, using the PaO2 measured with an FIO2 of 100%, the clinician can easily calculate the next desired FIO2 and quickly estimate the shunt fraction.
The degree of shunt with 100% FIO2 can be estimated by applying this general rule: The measured PaO2 is subtracted from 700 mm Hg. For each difference of 100 mm Hg, the shunt is 5%. A shunt of 25% should prompt the clinician to consider the use of PEEP.
Inadequate oxygenation despite the administration of 100% oxygen should lead to a search for complications of endotracheal intubation (eg, mainstem intubation) or positive-pressure breathing (pneumothorax). If such complications are not present, PEEP is needed to treat the intrapulmonary shunt pathology. Because only a few disease processes can create an intrapulmonary shunt, a clinically significant estimated shunt should narrow the potential source of hypoxemia to the following conditions:
- Alveolar collapse - Major atelectasis
- Alveolar filling with something other than gas - Lobar pneumonia
- Water and protein - ARDS
- Water - Congestive heart failure
- Blood - Hemorrhage
Positive end-expiratory pressure
PEEP is a mode of therapy used in conjunction with mechanical ventilation. At the end of mechanical or spontaneous exhalation, PEEP maintains the patient's airway pressure above the atmospheric level by exerting pressure that opposes passive emptying of the lung. This pressure is typically achieved by maintaining a positive pressure flow at the end of exhalation. This pressure is measured in centimeters of water.
PEEP therapy can be effective when used in patients with a diffuse lung disease that results in an acute decrease in functional residual capacity (FRC), which is the volume of gas that remains in the lung at the end of a normal expiration. FRC is determined by primarily the elastic characteristics of the lung and chest wall. In many pulmonary diseases, FRC is reduced because of the collapse of the unstable alveoli. This reduction in lung volume decreases the surface area available for gas exchange and results in intrapulmonary shunting (unoxygenated blood returning to the left side of the heart). If FRC is not restored, a high concentration of inspired oxygen may be required to maintain the arterial oxygen content of the blood in an acceptable range.
Applying PEEP increases alveolar pressure and alveolar volume. The increased lung volume increases the surface area by reopening and stabilizing collapsed or unstable alveoli. This splinting, or propping open, of the alveoli with positive pressure improves the ventilation-perfusion match, reducing the shunt effect.
After a true shunt is modified to a ventilation-perfusion mismatch with PEEP, lowered concentrations of oxygen can be used to maintain an adequate PaO2. PEEP therapy may also be effective in improving lung compliance. When FRC and lung compliance are decreased, additional energy and volume are required to inflate the lung. By applying PEEP, the lung volume at the end of exhalation is increased. The already partially inflated lung requires less volume and energy than before for full inflation.
When used to treat patients with a diffuse lung disease, PEEP should improve compliance, decrease dead space, and decrease the intrapulmonary shunt effect. The most important benefit of the use of PEEP is that it enables the patient to maintain an adequate PaO2 at a low and safe concentration of oxygen (<60%), reducing the risk of oxygen toxicity
Because PEEP is not a benign mode of therapy and because it can lead to serious hemodynamic consequences, the ventilator operator should have a definite indication to use it. The addition of external PEEP is typically justified when a PaO2 of 60 mm Hg cannot be achieved with an FIO2 of 60% or if the estimated initial shunt fraction is greater than 25%. No evidence supports adding external PEEP during initial setup of the ventilator to satisfy misguided attempts to supply prophylactic PEEP or physiologic PEEP.
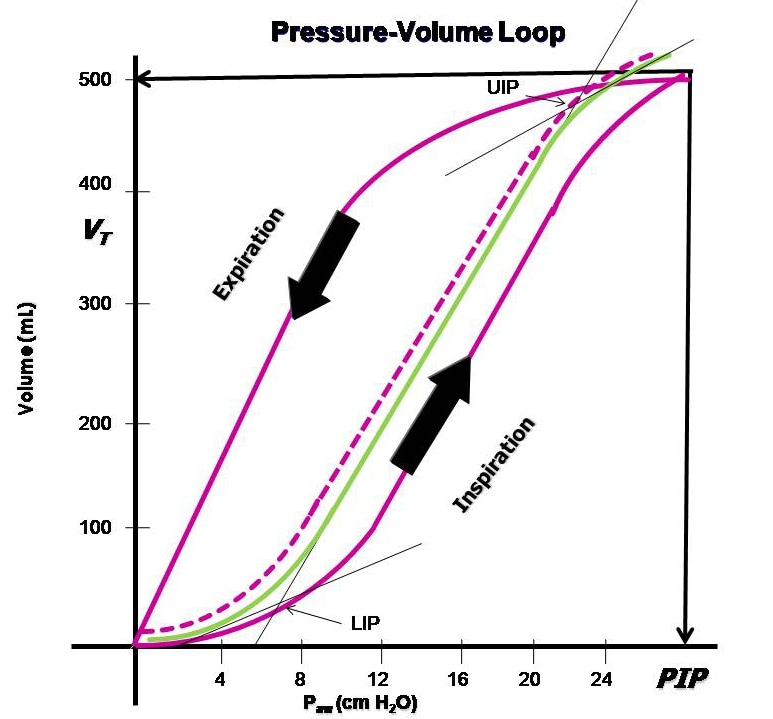
Many clinicians use the least-PEEP philosophy, which recommends using the lowest positive pressure that provides an adequate PaO2 with a safe FIO2. Another manner of selecting the optimal PEEP is based on identifying the low inflection point on the volume-pressure curve generated breath to breath by using modern mechanical ventilators. PEEP should be set 1-2 cm of water pressure above this measured low inflection point to obtain the optimal PEEP
Because PEEP basically resets the baseline of the pressure-volume curve, the peak and plateau pressures will be affected. The clinician should pay close attention to the status of these pressure measurements
Because PEEP basically resets the baseline of the pressure-volume curve, the peak and plateau pressures will be affected. The clinician should pay close attention to the status of these pressure measurements
Determination of the lower inflection point to estimate the best (optimal) positive end-expiratory pressure (PEEP) from the pressure-volume hysteresis curve.
Summary of initial ventilator setup
Initial settings for ventilation may be summarized as follows:
- Assist-control mode
- Tidal volume set depending on lung status
- Normal = 12 mL/kg ideal body weight
- COPD = 10 mL/kg ideal body weight
- ARDS = 6-8 mL/kg ideal body weight
- Rate of 10-12 breaths per minute
- FIO2 of 100%
- Sighs rarely needed
- PEEP only as indicated after first arterial blood gas determination, ie, shunt greater than 25%
- Inability to oxygenate with an FIO2 less than 60%
Adjustments and Withdrawal
Prone positioning
Prone positioning has been used in patients with ARDS and severe hypoxia and improves FRC, postural drainage of secretions, and ventilation-perfusion matching. Moving the intubated patient from the supine position to the prone position requires a coordinated effort from the nursing staff, respiratory therapists, and physicians to prevent inadvertent extubation or loss of various lines and tubes. Prone positioning may improve oxygenation in greater than 50% of such patients, but no survival benefit has been documented.
Sedation, protocols, and prophylaxis
Most patients receiving mechanical ventilation need sedation given by means of continuous infusion or scheduled dosing to help with anxiety and psychological stress inherent with this intervention. Daily interruption of sedation, when clinically allowable, decreases the number of days of mechanical ventilation. This sedation holiday helps the patient become reoriented and prevents the unintended prolonged effects of sedation. Such interruptions also help in assessing the patient for the appropriateness of weaning and hasten the transition to spontaneous respiration.
Studies have demonstrated that protocols driven by respiratory therapy safely decrease the number of ventilator days. These protocols allow the respiratory therapists to begin spontaneous breathing trials (SBTs) when they consider the patient a candidate for weaning.
Elevating the head of the patient's bed by greater than 30° decreases the risk of ventilator-associated pneumonia (VAP). Likewise, rates of VAP can be decreased with implementation of GI prophylaxis with histamine-2 blocking agents or proton-pump inhibitors, as well as deep vein thrombosis prophylaxis. Each of these measures should be undertaken in all patients receiving mechanical ventilation unless a contraindication is present.
PEEP adjustment
A PEEP level of less than 10 cm water rarely causes hemodynamic problems in the absence of intravascular volume depletion. The cardiodepressant effects of PEEP are often minimized with judicious intravascular volume support or cardiac inotropic support. Although peak pressure is related to the development of barotrauma, arterial hypotension is related to the mean airway pressure that may decrease venous return to the heart or decrease right ventricular function.
A PEEP level greater than 10 cm water is generally an accepted indication to monitor cardiac output by using a Swan-Ganz catheter. However, if the patient remains clinically stable with an adequate urine output, then hemodynamic monitoring may not be necessary. When PEEP greater than 10 cm water is necessary, the left atrial filling pressure can be estimated after an adjustment is made for the effect of the PEEP on the transducer of the catheter. The equation commonly used is LAP = PCWP - (PEEP/3), where LAP is left atrial pressure and PCWP is pulmonary capillary wedge pressure.
Withdrawal of PEEP from a patient should not be attempted in most clinical situations until the patient has achieved satisfactory oxygenation with an FIO2 of 40% or less. Formal weaning from PEEP is then undertaken by reducing the PEEP in 3- to 5-cm of water decrements while the hemoglobin-oxygen saturations are monitored. An unacceptable decrease in the hemoglobin-oxygen saturation should prompt the clinician to immediately reinstitute the last PEEP level that provided good hemoglobin-oxygen saturation.
When to withdraw mechanical ventilation
Weaning or, as some physicians prefer, "liberation from mechanical ventilation," is an important issue. Unnecessary delays in the withdrawal of mechanical ventilatory support increase the patient's risks for complications and increase the length of ICU stay and hospital costs. However, premature withdrawal from the ventilator can also be deleterious.
Weaning should be considered when the event that precipitated the patient's need for mechanical support is adequately addressed. Patients should be evaluated each day to determine if they are a candidate for weaning. Patients who may be able to support their own ventilation and oxygenation can often be recognized by assessing objective measurements or by asking the following questions:
- Is the process responsible for the patient's respiratory failure resolving or improving?
- Is the patient hemodynamically stable? Is the patient free of active cardiac ischemia or unstable arrhythmias, and vasopressor support absent or minimal?
- Is oxygenation adequate with a PaO2 of greater than 60 mm Hg with an FiO2 of less than 40% and a PEEP of less than 5 cm water?
- Are mental and neuromuscular statuses appropriate with the patient on minimal or no sedation? Does the patient have adequate strength of the respiratory muscles?
- Are the acid-base status and electrolyte status optimized?
- Is the patient afebrile?
- Are the patient's adrenal and thyroid functions adequate to allow for weaning?
Numerous weaning parameters can be used to help predict successful extubation. However, no weaning protocol is 100% accurate in predicting successful weaning and extubation. These weaning parameters must be tailored for each clinical scenario.
For instance, if the rapid, shallow breathing index (the respiratory rate/tidal volume, or frequency/tidal volume [f/Vt]) is less than 105, the patient is likely to be weaned from mechanical ventilation. The investigators who derived this number examined primarily middle-aged patients. However, data from follow-up studies of patients older than 70 years suggest that a slightly higher rapid, shallow breathing index of less than 130 may be acceptable.
These parameters give no insight into whether a patient can protect his or her airway or clear secretions. Clinical judgment and experience play a large role in the physician's decision to withdraw mechanical ventilatory support. If a patient cannot be extubated and/or if the results of the rapid, swallow breathing test are not satisfactory, the reason for the failure must be evaluated and treated.
Parameters commonly used to assess a patient's readiness to be weaned from mechanical ventilatory support include the following:
- Respiratory rate less than 25 breaths per minute
- Tidal volume greater than 5 mL/kg
- Vital capacity greater than 10 mL/k
- Minute ventilation less than 10 L/min
- PaO2/FIO2 greater than 200
- Shunt (Qs/Qt) less than 20%
- Negative inspiratory force (NIF) less than (more negative) -25 cm water
- f/Vt less than 105, or less than 130 in elderly patients
How to withdraw mechanical ventilation
Weaning from mechanical ventilation is intended to shift the work of breathing from the ventilator back to the patient over time. An issue separate from discontinuing ventilator support is determining if the patient can maintain his or her airway and be extubated safely. The weaning process must ensure the patient's safety while avoiding undue delay that might increase the risk of VAP.
The 3 general approaches to weaning are synchronized intermittent mandatory ventilation (SIMV), pressure-support ventilation (PSV), and an SBT.
In SIMV, breaths are either a mandatory ventilator-controlled breath or a spontaneous breath with or without pressure support. The original intent of SIMV was to let the patient's respiratory muscles rest during the mandatory breaths and to work during the spontaneous breaths Weaning is accomplished by decreasing the number of mandatory breaths, gradually increasing the workload of the respiratory muscles. Weaning is typically done by 2 breaths every 1–2 hours. The patient's heart rate, respiratory rate, and oxygen saturation indicate his or her ability to accept the work of breathing.
The pressure, volume, and flow to time waveforms for synchronized intermittent mandatory ventilation (SIMV).
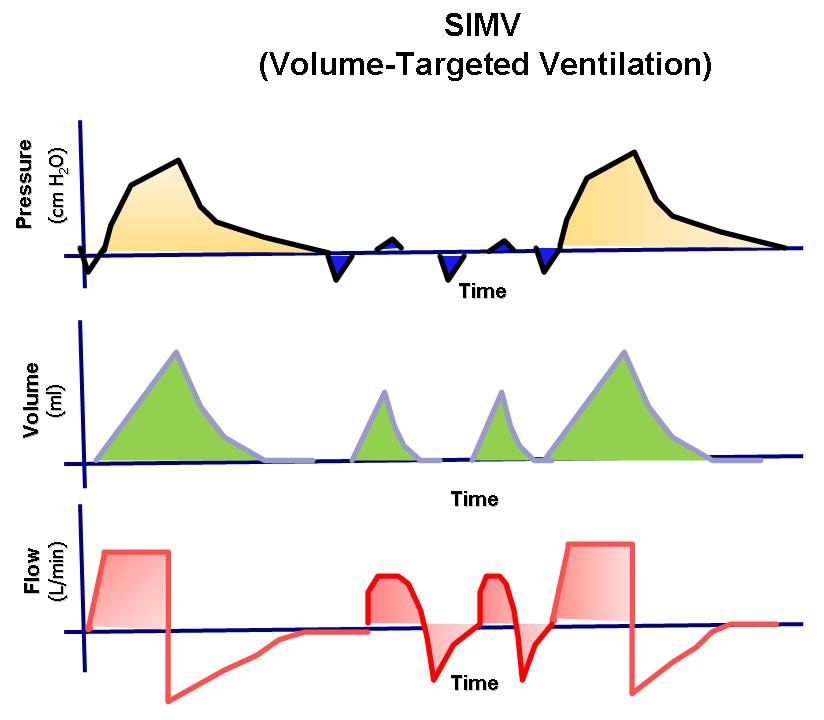
Evidence now suggests that the respiratory muscles are not able to rest during the mandatory breaths and that this mode may actually result in muscle fatigue and prolonged mechanical ventilation. Findings from randomized trials suggest that SIMV weaning delays extubation compared with PSV and SBT and that it should not be the primary mode of weaning in most patients. However, SIMV weaning does ensure that the patient receives some ventilatory support, and it may be favored in institutions where the staffing level of respiratory therapists is not optimal.
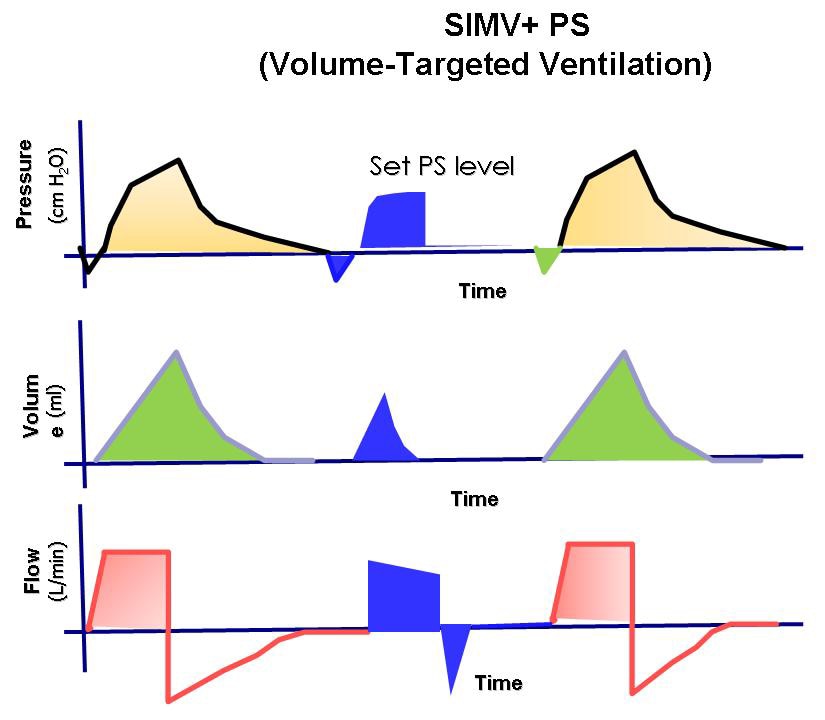
In PSV weaning, all breaths are spontaneous and combined with enough pressure support to ensure that each breath is a reasonable tidal volume. The pressure support lowers the work of breathing for the patient. Weaning is performed by gradually decreasing the amount of pressure support and by transferring an increased proportion of the work to the patient. This transfer is continued until the pressure support approaches 5-6 cm water. When the patient can tolerate this level of ventilatory support, extubation is usually successful. Studies have demonstrated that PSV weaning reduces the number of days on mechanical ventilation compared with SIMV alone. PSV can be used in conjunction with SIMV when a patient is weaned from mechanical ventilation . The coupling of these 2 modes is an especially attractive option in frail patients with underlying chronic illnesses.
The pressure, volume, and flow to time waveforms for synchronized intermittent mandatory ventilation (SIMV) with pressure-support ventilation.
The preferred method of weaning is the SBT. This is an attempt to gauge how the patient might do if he or she is immediately removed from the ventilator. This method is also referred to as the sink-or-swim trial. The key is to withdraw ventilatory support while oxygenation is continued.
The simplest form of SBT is the T-piece trial. The patient is disconnected from the ventilator, and the endotracheal or tracheostomy tube is hooked to a flow-by oxygen system, usually from the wall. The transition from the ventilator tubing to the new tubing attached to the wall oxygen outlet requires extra work and patient monitoring by the respiratory therapist.
The same assessment can be made by using the continuous positive-airway pressure (CPAP) mode while the patient is still connected to the ventilator. This is a relatively common method of assessing the patient's ability to do the work of breathing by himself or herself. Variations on this theme include adding a small amount of pressure and using a CPAP of 5 cm water or a CPAP of 0 but with a PSV of 5-6 cm water to offset the resistance from the artificial airway. To the authors' knowledge, no controlled studies have shown any superiority in assessing the outcomes of weaning between these approaches.
In some studies, approximately 80% of patients receiving mechanical ventilation do not require prolong weaning. This observation explains why SBT is both useful and practical. This approach has had the most success with weaning in randomized controlled trials. Therefore, it is a preferred approach to removing patients from mechanical ventilation.
The SBT should last 30-90 minutes. At the end of the SBT, the patient should be evaluated for possible extubation, as his or her blood pressure, respiratory rate, heart rate, and gas exchange are also considered. An SBT should be performed only once a day. Several SBTs a day offer no benefit.
Complications of Mechanical Ventilation
Complications can occur at any stage of mechanical ventilation and are sometimes life threatening.
Complications of intubation
Complications that can occur during placement of an endotracheal tube include upper airway and nasal trauma, tooth avulsion, oral-pharyngeal laceration, laceration or hematoma of the vocal cords, tracheal laceration, perforation, hypoxemia, and intubation of the esophagus. Inadvertent intubation of the right mainstem bronchus is reported in 3-9% of all intubations in adults. Aspiration rates are 8–19% in intubations performed in adults without anesthesia. Sinusitis, tracheal necrosis or stenosis, glottic edema, and VAP may occur with prolonged use of endotracheal tubes.
Additionally, the following guidelines from the American Association for Respiratory Care may be helpful: . Additionally, Solsona et al reported that observation of intercostal retraction after adding dead space may help in the detection of susceptibility to extubation failure.
Additionally, the following guidelines from the American Association for Respiratory Care may be helpful: . Additionally, Solsona et al reported that observation of intercostal retraction after adding dead space may help in the detection of susceptibility to extubation failure.
Ventilator-induced lung injury
With ventilator-induced lung injury, the alveolar epithelium is at risk for both barotrauma and volutrauma.
Barotrauma
Barotrauma refers to rupture of the alveolus with subsequent entry of air into the pleural space (pneumothorax) and/or the tracking or air along the vascular bundle to the mediastinum (pneumomediastinum). The true prevalence of barotrauma is difficult to establish, and reports suggest a rate of 6-25%. Large tidal volumes and elevated peak inspiratory and plateau pressures are risk factors. Studies in patients with ARDS demonstrated that the severity of the underlying lung pathology is a better predictor of barotrauma than the observed peak inspiratory pressure. Even so, peak inspiratory pressures of less than 45 mm Hg and plateau pressures of less than 30-35 mm Hg are recommended.
The inspiratory-to-expiratory ratio can be adjusted by increasing the inspiratory flow rate, by decreasing the tidal volume, and by decreasing the ventilatory rate. Attention to the inspiratory-to-expiratory ratio is important to prevent barotrauma in patients with obstructive airway disease (eg, asthma, chronic obstructive pulmonary disease).
Also see Barotrauma and Mechanical Ventilation.
Volutrauma
Volutrauma refers to the local overdistention of normal alveoli. Volutrauma has gained recognition over the last 2 decades and is the impetus for the lung protection ventilation with low tidal volumes of 6–8 mL/kg. CT studies have demonstrated that ARDS has a heterogeneous pattern of lung involvement. Abnormal consolidated lung is dispersed within normal lung tissue. When a mechanical ventilation breath is forced into the patient, the positive pressure tends to follow the path of least resistance to the normal or relatively normal alveoli, potentially causing overdistention. This overdistention sets off an inflammatory cascade that augments or perpetuates the initial lung injury, causing additional damage to previously unaffected alveoli. The increased local inflammation lowers the patient's potential to recover from ARDS. The inflammatory cascade occurs locally and may augment the systemic inflammatory response as well.
Another aspect of volutrauma associated with positive ventilation is the shear force associated with the opening and closing effects on collapsible alveoli. This has also been linked to worsening the local inflammatory cascade. PEEP prevents the alveoli from totally collapsing at the end of exhalation and may be beneficial in preventing this type of injury. Since volutrauma was recognized, a lung-protective ventilation strategy is recommended in all patients with ARDS or acute lung injury.
Oxygen toxicity
Oxygen toxicity is a function of increased FIO2 and its duration of use. Oxygen toxicity is due to the production of oxygen free radicals, such as superoxide anion, hydroxyl radical, and hydrogen peroxide. Oxygen toxicity can cause a variety of complications ranging from mild tracheobronchitis, absorptive atelectasis, and hypercarbia to diffuse alveolar damage that is indistinguishable from ARDS.
No consensus has been established for the level of FIO2 required to cause oxygen toxicity, but this complication has been reported in patients given a maintenance FIO2 of 50%. The clinician is encouraged to use the lowest FIO2 that accomplishes the needed oxygenation.
The medical literature suggests that the clinician should attempt to attain an FIO2 of 60% or less within the first 24 hours of mechanical ventilation. If necessary, PEEP should be considered a means to improve oxygenation while a safe FIO2 is maintained. When PEEP is effective and not contraindicated because of hemodynamics, the patient can often be oxygenated while the risks of oxygen toxicity are limited.
The medical literature suggests that the clinician should attempt to attain an FIO2 of 60% or less within the first 24 hours of mechanical ventilation. If necessary, PEEP should be considered a means to improve oxygenation while a safe FIO2 is maintained. When PEEP is effective and not contraindicated because of hemodynamics, the patient can often be oxygenated while the risks of oxygen toxicity are limited.
Ventilator-associated pneumonia
VAP is a life-threatening complication with mortality rates of 33-50%. It is reported to occur in 10-25% of patients given mechanical ventilation. The risk of VAP is highest immediately after intubation. VAP is estimated to occur at a rate of 3% per day for the first 5 days, 2% per day for next 5 days, and 1% per day thereafter. VAP occurs more frequently in trauma, neurosurgical, or burn units than in respiratory units and medical ICUs.
VAP is defined as a new infection of the lung parenchyma that develops within 48 hours after intubation. The diagnosis can be challenging. VAP should be suspected when a new or changing pulmonary infiltrate in seen in conjunction with fever, leukocytosis, and purulent tracheobronchial secretions. However, many diseases can cause this clinical presentation. Examples include aspiration pneumonitis, atelectasis, pulmonary thromboembolism, drug reactions, pulmonary hemorrhage, and radiation-induced pneumonitis. Qualitative and quantitative cultures of protected brush and bronchoalveolar lavage specimens may help with the diagnosis, but the utility of these techniques is still debated.
Microorganisms implicated in VAP that occurs in the first 48 hours after intubation are flora of the upper airway, including Haemophilus influenza and Streptococcus pneumonia. After this early period, gram-negative bacilli such as Pseudomonas aeruginosa; Escherichia coli; and Acinetobacter, Proteus, and Klebsiella species predominate. Staphylococcus aureus, especially methicillin-resistant S aureus (MRSA), typically becomes a major infective agent after 7 days of intubation and mechanical ventilation. Most of the medical literature recommends initial therapy with broad-spectrum antibiotics that cover pathogens resistant to multiple drugs until the sensitivities of the causative organism are identified. Knowledge of organisms that cause VAP in the individual ICU and the pattern of antibiotic resistance is imperative. Choices of antibiotics should be tailored to the microorganisms and the antimicrobial resistance observed in each ICU.
Intrinsic PEEP, or auto-PEEP
Intrinsic PEEP or auto-PEEP is a complication of mechanical ventilation that most frequently occurs in patients with COPD and/or asthma who require prolonged expiration. These patients may have difficulty in totally exhaling the ventilator-delivered tidal volume before the next machine breath is delivered. When this problem occurs, a portion of each subsequent tidal volume may be retained in the patient's lungs, a phenomenon sometimes referred to as breath stacking If this goes unrecognized, the patient's peak airway pressure may increase to a level that results in barotrauma, volutrauma, hypotension, patient-ventilator dyssynchrony, or death.
The flow to time waveform demonstrating auto–positive end-expiratory pressure (auto-PEEP).
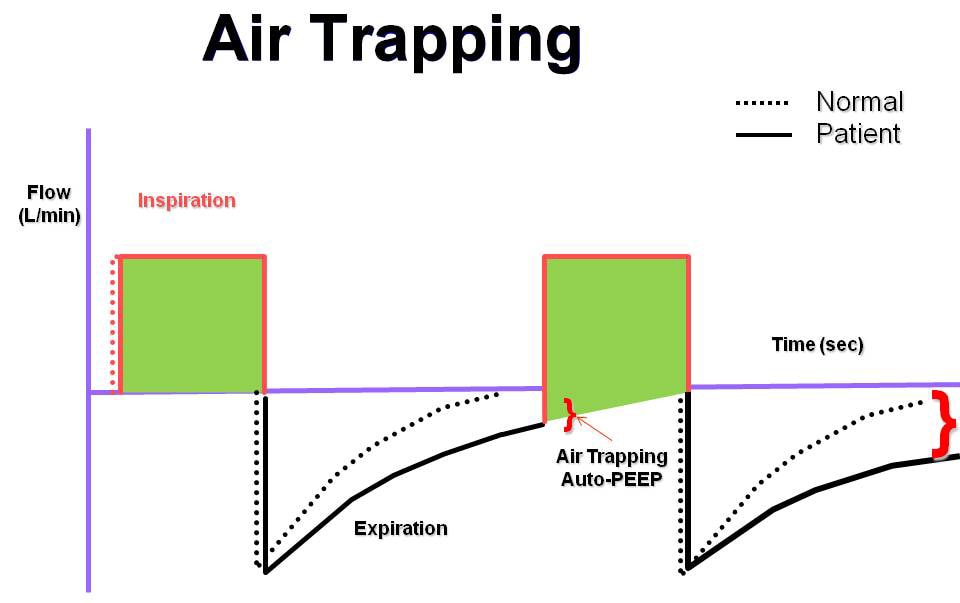
Manometry performed by using an esophageal balloon to record changes in pleural pressure is the most accurate way to recognize intrinsic PEEP. However, this technology is not available at most institutions. Therefore, clinicians must anticipate this complication and carefully monitor the measured peak airway pressure. When intrinsic PEEP is diagnosed, the patient should temporarily be released from mechanical ventilation to allow for full expiration. The ventilator can then be adjusted to shorten inspiration by decreasing the set tidal volume or by increasing the inspiratory flow rate.
Cardiovascular effects
Mechanical ventilation always has some effect on the cardiovascular system. Positive-pressure ventilation can decrease preload, stroke volume, and cardiac output. Positive-pressure ventilation also affects renal blood flow and function, resulting in gradual fluid retention. The incidence of stress ulcers and sedation-related ileus is increased when patients receive mechanical ventilation. In fact, mechanical ventilation is a primary indication for GI prophylaxis. Positive pressure maintained in the chest may decrease venous return from the head, increasing intracranial pressure and worsening agitation, delirium, and sleep deprivation. Alternative Modes of Mechanical Ventilation
In the last 2 decades, several modes of ventilation have emerged from the successful marriage of the ventilator and computer technology. Staying abreast of emerging ventilator modifications can be a formidable and ongoing challenge for physicians.
Dual-control ventilation modes were designed to combine the advantages of volume-control ventilation (guaranteed minute ventilation) with pressure-control ventilation (rapid, variable flow at a preset or limited peak airway pressure). These dual-control modes attempt to increase the safety and comfort of mechanical ventilation. Although this new technology seems promising, no findings from randomized trials indicate improved patient outcomes (including mortality).
Dual-control, breath-to-breath, pressure-limited, time-cycled ventilation
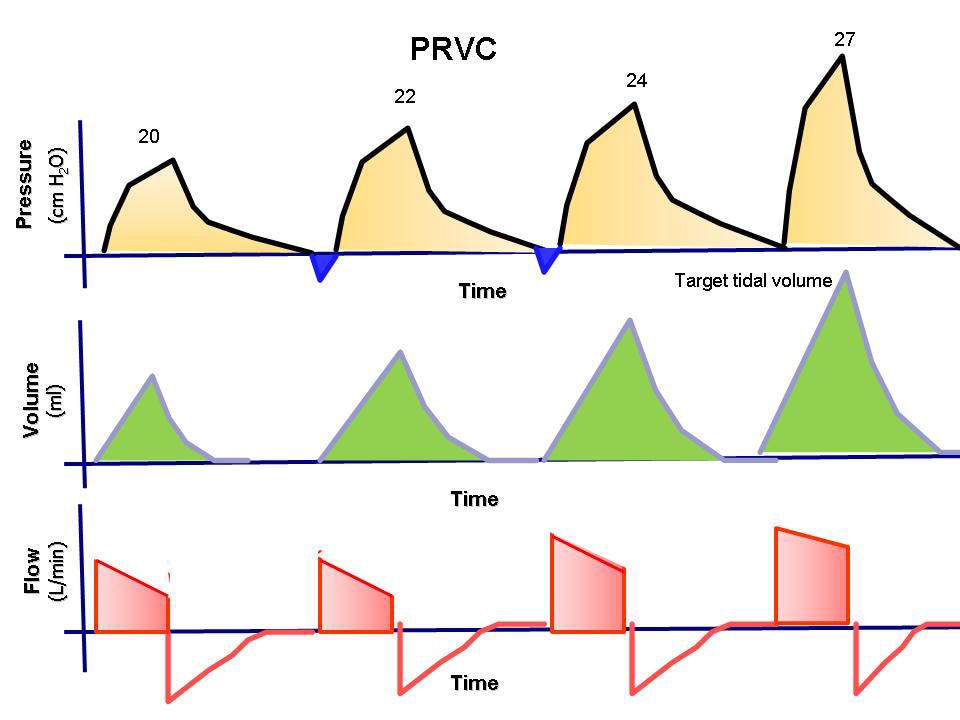
This mode has been called pressure-regulated volume-control (PRVC), adaptive pressure ventilation, auto-flow, volume-control +, or variable-pressure control ventilation according to various commercial ventilators. This mode is under the dual control of pressure and volume. The physician presets a desired tidal volume, and the ventilator delivers a pressure-limited (controlled) breath until that preset tidal volume is achieved. The breath is essentially like a conventional pressure-controlled ventilation breath, but the ventilator can guarantee a predetermined minute ventilation.
Breath to breath, the inspiratory pressure is automatically adjusted down or up according to the patient's lung compliance and/or resistance to deliver a preset tidal volume. The ventilator monitors each breath and compares the delivered tidal volume with the set tidal volume. If the delivered volume is too low, it increases the inspiratory pressure on the next breath. If it is too high, it decreases the inspiratory pressure. This adjustment gives the patient the lowest peak inspiratory pressure needed to achieve a preset tidal volume. The advantage of this mode is that it gives the physician the opportunity to deliver minimum minute ventilation at the lowest peak airway pressures possible .
The pressure, volume, and flow to time waveforms for pressure-regulated volume-controlled ventilation.
Dual-control breath-to-breath, pressure-limited, flow-cycled ventilation
This mode has been called volume-support ventilation (VSV) or variable-pressure-support according to which ventilator is used. This mode is a combination of PSV and volume-control ventilation. Like PSV, the patient triggers every breath, controlling his or her own respiratory frequency and inspiratory time. This mode delivers a breath exactly like conventional PSV, but the machine can guarantee minute ventilation. The pressure support is automatically adjusted up or down according to the patient's lung compliance and/or resistance to deliver a preset tidal volume.
This mode is similar to the dual-control breath-to-breath, pressure-limited, time-cycled ventilation except that it is flow cycled, which means that the patient determines the respiratory rate and inspiratory time. The mode cannot be used in a patient who lacks spontaneous breathing effort.
Volume support has also been marketed as a self-weaning mode. Therefore, as the patient's effort and/or compliance or resistance improve, pressure support is automatically titrated down without the need for input from a physician or therapist.
A number of potential problems can arise. If the patient's metabolic demand increases, raising the tidal volume, the pressure support decreases to provide less ventilatory support when the patient needs it most. The clinician must be aware that, as the level of pressure support drops, mean airway pressure decreases; this effect may possibly result in hypoxemia. The other concern is that the tidal volume must be correctly set to the patient's metabolic needs. If the tidal volume is set too high, weaning is delayed. If it is set too low, the work of breathing may be more than what the patient can reasonably accomplish.
Automode and variable support or variable-pressure control
This mode is basically the combination of the 2 modes described above. If the patient has no spontaneous breaths, the ventilator is set up in the PRVC mode. However, when the patient takes 2 consecutive breaths, the mode is switched to VSV. If the patient becomes apneic for 12 seconds, the ventilator switches back to PRVC mode.
Automode and variable support or variable-pressure control was designed for automatic weaning from pressure control to pressure support depending on the patient's effort. This ventilatory mode can also be used in conventional volume control and volume support; again, the mode depends on the patient's effort. To the authors' knowledge, no randomized trials have been conducted to evaluate this automode, and no evidence suggests that this type of weaning is more effective than conventional weaning.
Dual control within a breath
This mode has been called volume-assured pressure support or pressure augmentation according to various manufacturers. This mode can switch from pressure control to volume control within a single specific breath cycle. After a breath is triggered, rapid and variable flow creates pressure to reach the set level of pressure support. The tidal volume that is delivered from the machine is monitored. If the tidal volume equals the minimum set tidal volume, the patient receives a typical pressure-supported breath, which makes this mode essentially like volume support. However, if the tidal volume is less than the set tidal volume, the ventilator switches to a volume-controlled breath with constant flow rate until the set tidal volume is reached.
One study compared volume-assured pressure support with simple assist-control volume support and showed a 50% reduction in the work of breathing, lowered airway resistance, and lowered intrinsic PEEP. However, because of its complexity, this mode is rarely used.
Automatic tube compensation
This mode is specifically used for weaning and is designed to overcome the resistance of the endotracheal tube by means of continuous calculations. These calculations deal with known resistive coefficients of the artificial airway (size and length), tracheal pressures, and measurement of instantaneous flow. These calculations allow the ventilator to supply the appropriate pressure needed to overcome this resistance throughout the entire respiratory cycle. To the authors' knowledge, no studies have proven that this mode is any better than SBTs.
Proportional assist ventilation4
This mode was designed to decrease the work of breathing and improve patient-ventilator synchrony. The mode adjusts airway pressure in proportion to the patient's effort. Unlike other modes in which the physician presets a specific tidal volume or pressure, proportional assist ventilation (PAV) lets the patient determine the inspired volume and the flow rate. This mode requires continuous measurements of resistance and compliance to determine the amount of pressure to give. The support given is a proportion of the patient's effort and is normally set at 80%. This support is always changing according to patient's effort and lung dynamics. If the patient's effort and/or demand are increased, the ventilator support is increased, and vice versa, to always give a set proportion of the breath. The patient's work of breathing remains constant regardless of his or her changing effort or demand (see Media File 12).
The pressure, volume, and flow to time waveforms for proportional-assist ventilation.
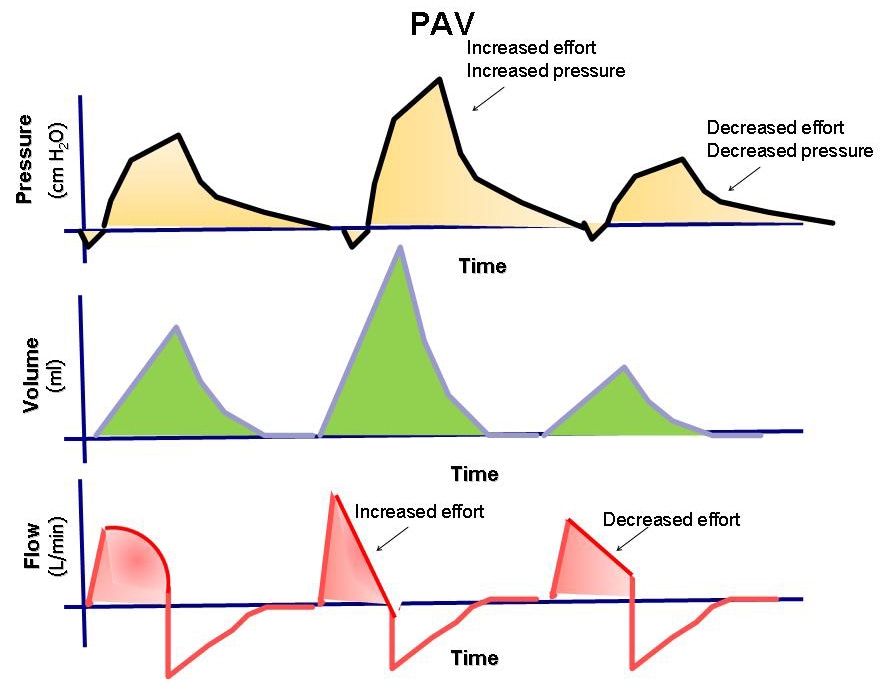
This mode can be used only in patients with spontaneous respiratory efforts. PAV has promise, but the US Food and Drug Administration (FDA) has not approved it for commercial use.
Airway pressure–release ventilation
Bilevel, or biphasic, ventilation is a relatively new mode of ventilation that has recently gained popularity. The ventilator is set at 2 pressures (high CPAP, low CPAP), and both levels are time cycled. The high pressure is maintained for most of the time, while the low pressure is maintained for short intervals of usually less than 1 second to allow exhalation and gas exchange to occur. The patient can breathe spontaneously during high or low pressure (see Media File 13). This mode has the benefit of alveolar recruitment. Its disadvantage is that the tidal volume is variable. The clinician must be constantly aware of the patient's minute ventilation to prevent severe hypercapnia or hypocapnia.
The pressure, volume, and flow to time waveforms for airway pressure–release ventilation.
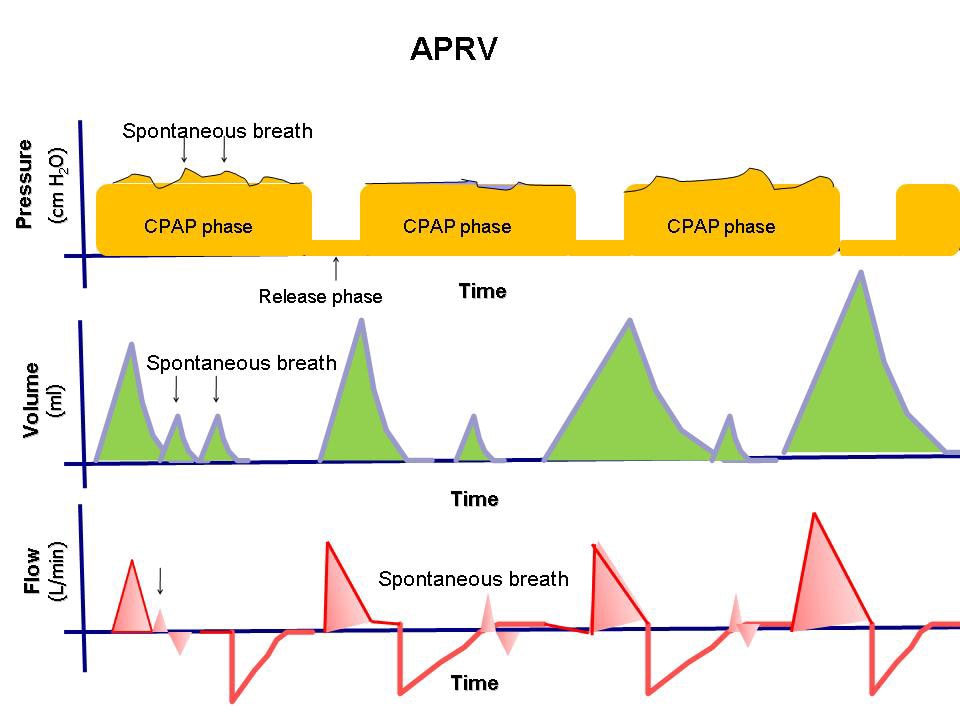
Conclusion
With computer feedback systems, many modern ventilators allow the operator to make fine adjustments in tidal volume, airway pressures, and the timing of the respiratory cycle. The desired result is improved ventilator-patient interaction and limitation of ventilator-induced lung injury. These newer methods of mechanical ventilation are often based on attractive physiologic hypotheses, and they are interesting to implement. Each method has its proponents, but objective evidence has failed to show that any of the alternative methods of ventilation is more successful than conventional mechanical ventilation with proper attention to tidal volume. Most clinicians use alternative methods of ventilation only in cases when conventional mechanical ventilation has failed.
Clinical Trials
- Weaning Children From Mechanical Ventilation:Computer-Driven System Versus Usual Care
- Pneumonectomy and Protective Mechanical Ventilation
- Music Therapy for Patients Being Weaned From Mechanical Ventilation
Multimedia
 | Media file 1: An example of the Drinker and Shaw negative-pressure ventilator (iron lung). |

 | Media file 2: The pressure, volume, and flow to time waveforms for assist-control ventilation. |
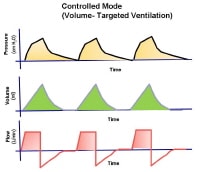 | Media file 3: The pressure, volume, and flow to time waveforms for controlled ventilation. |
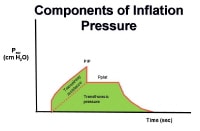 |
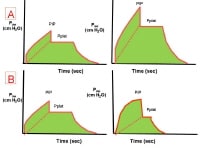 | Media file 5: The effects of increased airway resistance (A) and decreased respiratory system compliance on the pressure-time waveform. |
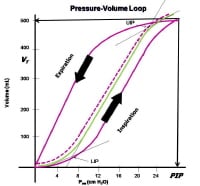 | Media file 6: Determination of the lower inflection point to estimate the best (optimal) positive end-expiratory pressure (PEEP) from the pressure-volume hysteresis curve. |
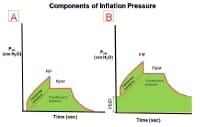 | Media file 7: The effect of positive end-expiratory pressure (PEEP) on the pressure-time inflation curve. |
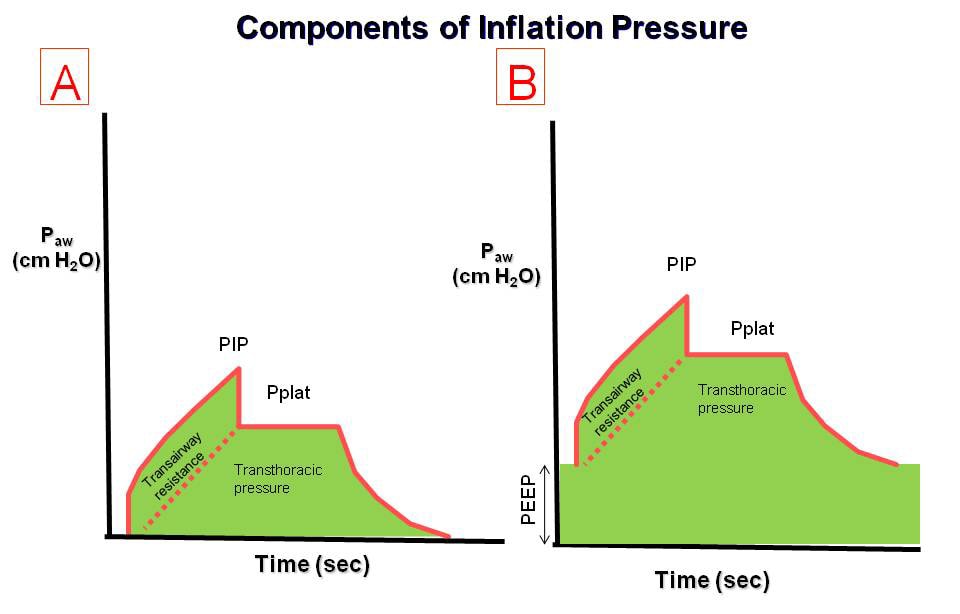
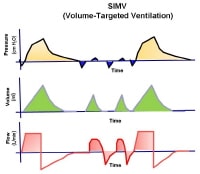 | Media file 8: The pressure, volume, and flow to time waveforms for synchronized intermittent mandatory ventilation (SIMV). |
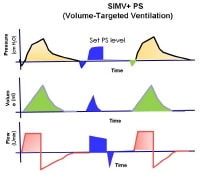 | Media file 9: The pressure, volume, and flow to time waveforms for synchronized intermittent mandatory ventilation (SIMV) with pressure-support ventilation. |
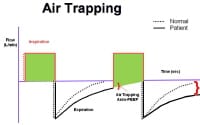 | Media file 10: The flow to time waveform demonstrating auto–positive end-expiratory pressure (auto-PEEP). |
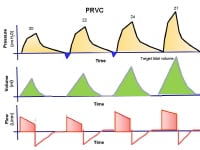 | Media file 11: The pressure, volume, and flow to time waveforms for pressure-regulated volume-controlled ventilation. |
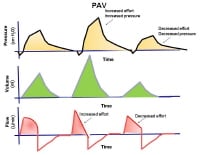 | Media file 12: The pressure, volume, and flow to time waveforms for proportional-assist ventilation. |
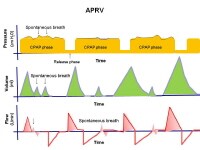 | Media file 13: The pressure, volume, and flow to time waveforms for airway pressure–release ventilation. |
Keywords
mechanical ventilation, conventional respiratory support, positive pressure ventilation, positive-pressure ventilation, negative-pressure ventilation, negative pressure ventilation, iron lung, cuirass, shell unit, acute lung injury, chronic obstructive lung disease, apnea, respiratory arrest, neuromuscular disease, chronic obstructive pulmonary disease, COPD, acute respiratory distress syndrome, ARDS, permissive hypercapnia, iron lung
Subscribe to:
Posts (Atom)

















